Supreme Court Judgment on Novartis Case Vindication of Left’s principled position in 2005
06/04/2013
On 26th December 2004 the then UPA-I Government promulgated an ordinance — The Patents (Amendment) Ordinance, 2004.
The ordinance was issued by the government to change the then existing Indian Patents Act in order to make it conform to the agreement on Trade Related Intellectual Property Rights (TRIPs), that India had signed as part of the World Trade Organisation (WTO) agreement in 1994. The Amended Act contained in the ordinance was to replace the earlier 1970 Act that had been widely recognized as a key reason why India had become a centre for production of affordable versions of new drugs – prompting many to term India as the ‘pharmacy of the South’, which supplied low-cost affordable drugs to a very large number of low and middle income countries in Asia, South America and Africa.
The ordinance had to be ratified by Parliament within 6 months. If the Indian Parliament had done so, we would not have been discussing the recent judgment by the Supreme Court of India against the claim of a patent on an important anti-cancer drug (Imatinib), manufactured by the Swiss Multinational, Novartis. Instead of ratifying the ordinance the Indian Parliament introduced, in 2005, several measures to safeguard continued production of new medicines by Indian companies, even in cases when in other parts of the world MNCs had patented these drugs and held a monopoly over their production and sales. One of the important clauses introduced by the Indian Parliament was a new section – section 3(d). This section lies at the heart of the litigation that Novartis has been pursuing for seven years, and it is this section which has been instrumental in the refusal of the patent by the Supreme Court of India.

The recent Supreme Court judgment is the fourth time that Novartis has been refused a patent on Imatinib in India – initially by the Patent office in 2006, and subsequently by the Patent Appellate Board and the Chennai High Court. Before we trace how these events unfolded, the story of how the Parliament managed to enact provisions that safeguarded public health to some extent in spite of the constraints of the TRIPS agreement needs to be told again.
The story of Patents Amendment Act of 2005 retold
The Patents Amendment Ordinance of 2004 was a public health disaster. It was drafted keeping in mind the interests of Multinational Corporations and was clearly aligned to the neo-liberal economic policies of the Government. If ratified by Parliament it would have made it impossible for Indian companies to continue producing cheaper versions of new drugs. Interestingly the ordinance had not been drafted by the UPA I Government – the government of the day had merely introduced a draft originally drafted by its predecessor, the BJP led NDA government! So in the end of 2004 there was a consensus between the principal bourgeois parties – the Congress and the BJP – as regards how Indian’s Patent Act would be amended. Given that the Congress led UPA I government had merely reproduced the earlier BJP government’s draft, there were obvious reasons to believe that the ordinance would sail through Parliament. In the then political spectrum only the Left Parties stood firmly against the 2004 ordinance, but they were not – on the basis of their own strength – in a position to defeat the
designs of the Congress-BJP combine.
The situation changed dramatically in early 2005 for reasons that had nothing to do with the issue at hand. In early 2005 the BJP was engaged in a bitter tussle with the Congress in Bihar and Jharkhand over formation of ministries in these two states. The BJP did a volte face and announced that it would not support the passage of the Patents Ordinance of 2004 in Parliament. This ploy of the BJP was not a consequence of any principled opposition to the ordinance, but was clearly an attempt to embarrass the government. But the BJP’s opposition to its own draft (!) provided the Left with an opportunity to intervene decisively. The Congress was now forced to seek the Left’s support in Parliament. It is this conjuncture of circumstances that provided the Left the opportunity to introduce several amendments to the 2004 ordinance. The recent Supreme Court judgment refers to this process and states: “As the deliberations were going on in Parliament, negotiations were also held between the ruling party and some of the opposition parties, in course of which certain amendments were suggested in the Bill”. The negotiations between the Left and the government was long and tortuous, with the Government trying to obstruct at every step the introduction of progressive pro-health and pro-people amendments. In the face of such strong resistance the Left was able to force the inclusion of several changes in the 2004 ordinance. At the end, twelve important amendments were made to the 2004 ordinance, including the insertion of section 3(d), mentioned earlier.
The Left was able to force through these changes not just because of the opportunity it seized in March 2005, but also because of the consistent position it had adopted on the issue since the 1980s. While MPs belonging to the Left were negotiating with the Government in 2005, Left mass organisations were engaged in protests and demonstrations on the issue all over the country. It was the combined strength of the Left’s principled position inside Parliament and the mass mobilisation on the issue that took place outside, that forced the government’s hand.
Misplaced allegations of sell-out by the Left in 2005
There was another curious aside to the events that led to the Parliament adopting the new Patents Act of 2005. When the Act was adopted in 2005, a section of NGOs — including some influential international NGOs involved in the Access to Medicines Campaign — accused the Left of having sold out! They argued that the Left should not have allowed any amendments to the 1970 Patent Act (the 1970 Act did not recognize Patents on medicinal products at all). While this came across as very radical posturing, what it did not take into account was that it was only the Left that had firmly opposed the TRIPS agreement under the WTO since the 1980s. The international NGOs, and their counterparts in the country, have played an important role in mobilizing against use of patents by MNCs to restrict access to life saving and essential medicines in the past decade and a half. Unfortunately they were nowhere part of the debate when India and other developing countries signed the TRIPS agreement in 1994. The actual sellout took place in 1994, and at that time it was only the Left in India – which made common cause with the domestic industry –which had taken a consistent position against a global patent system that forced countries like India to change their Patent Act. It was not an accident that India was the only country of significance that used the entire ten year transition period before changing its law. The ten year transition period was available to all developing countries, meaning they were allowed the option of finally amending their act by December 2004, though the TRIPS agreement came into force in December 1994. However countries such as Brazil amended their act right after the TRIPS agreement and did not wait till 2004 to do so. That India was the last hold out was a consequence of the consistent position and its mobilisation on the issue, that started right from the start of the Uruguay round of negotiations in 1986. It is interesting that many of the same NGOs and some of their vocal spokespersons now claim the 2005 Patents Act as a victory for ‘civil society’ and the Indian Act as a model Act. The Left has never claimed that the present Indian Act is ideal, but it can legitimately claim that it was the best that it could achieve given the political circumstances in 2005.
Novartis and its battles in Indian Courts
Let us now turn to the Novartis judgment and its significance today. Imatinib mesylate has been patented in many countries by the Swiss MNC, Novartis, which sells the drug under the Brand name of Glivec. In India, the initial patent application for the medicine was rejected by the patent office in 2006. Novartis persisted in its efforts to get a patent and appealed to the Patent Appellate Board. When the Board rejected Novartis’ application again, the company challenged the decision in the Chennai High Court. It also challenged section 3(d) of the Indian Patents Act — a provision that had been cited by the Patent office while rejecting the Glivec patent application. The Chennai high court rejected both the appeals, which led to Novartis bringing its appeal to the Supreme Court of India.
The original patent on imatinib was filed by Novartis in 1993 for the ‘amorphous free base’ molecule of the chemical, Imatinib Mesylate. An amorphous substance is what exists in nature and is usually a mixture of different variants. In the 1998 Novartis filed a patent application in India for the Beta crystalline variant of the molecule, which is derived from the amorphous substance that they had earlier patented. They also claimed that the Beta crystalline variety is better absorbed by the body. The 1993 patent was not recognized in India as at that time Indian law did not allow patenting of medicines. When the law was changed in 2005, Novartis pressed for acceptance of its patent application for the Beta crystalline variety of the salt. The patent office rejected the patent and held that the invention claimed was anticipated by prior publication; that the invention claimed by Novartis was obvious to a person skilled in the art; and further that the patentability of the alleged invention was disallowed by section 3(d) of the Indian Patent Act.
Novartis’ subsequent appeals in the Patent appellate board and Chennai high court were rejected. The appellate board, while rejecting the patent again said: “Since India is having a requirement of higher standard of inventive step by introducing the amended section 3(d) of the Act, what is patentable in other countries will not be patentable in India. As we see, the object of amended section 3(d) of the Act is nothing but a requirement of higher standard of inventive step in the law particularly for the drug/pharmaceutical substances.” Novartis also challenged Section 3(d) of the Indian Act in the High Court, claiming that it was in violation of India’s obligations at the WTO. The Chennai high court pointed out that domestic courts cannot be asked to give an opinion regarding international treaties and obligations, and Novartis should take its complaint to the dispute settlement mechanism in the WTO. Novartis, has never done so and clearly Section 3(d) does not violate international obligations.
In the Supreme Court Novartis challenged the interpretation of Section 3(d). This section stipulates that trivial changes in existing molecules cannot be candidates for fresh patenting. Such trivial patenting (known as ‘evergreening’) is an old ploy used by drug companies to extend their monopoly. Companies first apply for a patent for the basic molecule and then attempt to extend the life of their monopoly by subsequently applying for fresh patents after a few years on as slightly different version of the original molecule. Such changes do not qualify for a patent under the Indian Act as they would have been anticipated (would have been obvious) to a person skilled in the art – thus it does not constitute real innovative activity.
In its appeal to the Supreme Court, Novartis argued that section 3(d) had not being properly interpreted. The section says that minor variations in an existing molecule cannot be patented unless there is a ‘significant’ enhancement in efficacy of the medicine. Novartis claimed that since the Beta variant is better absorbed – i.e. it has better ‘bioavailibility’ (by about 30%) it constitutes a significant therapeutic enhancement. It is interesting to note here that the patent office, while rejecting the company’s patent application, had stated that anybody trained in chemistry would know that an amorphous salt is made up of different variants, and it is common knowledge that the variant are likely to have slightly different properties.
The Supreme Court Judgment and its implications
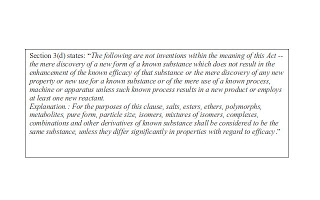
The Supreme Court in its judgment opined: “The subject product, that is, beta crystalline form of Imatinib Mesylate, is thus clearly a new form of a known substance, i.e., Imatinib Mesylate, of which the efficacy was well known. It, therefore, fully attracts section 3(d) and must be shown to satisfy the substantive provision and the explanation appended to it”. The judgment further goes on to say: “In whatever way therapeutic efficacy may be interpreted, this much is absolutely clear: that the physico-chemical properties of beta crystalline form of Imatinib Mesylate … may be otherwise beneficial but these properties cannot even be taken into account for the purpose of the test of section 3(d) of the Act, since these properties have nothing to do with therapeutic efficacy”. The judgment also addressed the claim of increased bio-availability by stating: “No material has been offered to indicate that the beta crystalline form of Imatinib Mesylate will produce an enhanced or superior efficacy (therapeutic) on molecular basis than what could be achieved with Imatinib free base….”.
Novartis has consistently played the victim in the Gilivec case. It continues to say that it was not fighting the case to make money but to uphold the principle that it deserves credit for the investment it has made in research to develop the drug. What Novartis does not tell us is that Glivec was granted ‘orphan drug’ status in the United States and was therefore eligible for tax rebates equal to half the cost of clinical testing (the major cost for drug development). Brian Druker, one of the scientists involved in developing Imatinib while working in Oregon Health and Science University Cancer Institute wrote in a signed article in livemint in 2007: “Many scientists, if not most of those I have collaborated with in these settings, are engaged in research primarily motivated by the pursuit of knowledge as a means to help patients. For many of these scientists it is, therefore, of great concern that the results of their efforts can’t reach patients and save lives because of pricing strategies and patent policies such as ‘patent evergreening’ (minor changes to existing molecules designed to extend patent monopolies) used by partners further down the drug development process”. Druker has again reiterated this position recently (in a comment to the Times of India) in the light of the Supreme court judgment.
Novartis had challenged a very important part of the the Indian Patent Act and its attempt to balance the rights of patent holders with the needs of the Indian people for access to treatment that is affordable. Section 3(d) of the Act has been used several times by the Indian patent office to deny patents for other trivial inventions, especially in the case of HIV/AIDS medicines. If Novartis’ appeal was upheld applicability of section 3(d) would have been seriously compromised, leading to the possible reopening of a number of rejected patent applications. It could also have opened the door for a flood of applications, many of which were not filed by companies because of the existence of Section 3(d). The Novartis judgment, thus, has implications for access to medicines not just for leukemia patients but for a whole range of patients — located not just in India but in over a hundred countries in Asia, Latin America and Africa — who are today able to access cheaper drugs made by Indian companies.