Nefarious Design to Legitimise Exorbitant Prices
04/01/2012
The Government has recently made public the “Draft National Pricing Pharmaceutical Policy, 2011” The circulation of the draft policy, supposedly to make medicines more affordable, comes in a situation where studies show that out-of-pocket medical costs push over 2% of the population below the poverty line in one year. A major part of expenditure on health in India, that people have to meet from their own resources, goes towards buying medicines. This is so because the government spends too little on health care and medicine prices are too high. Unlike in countries with well developed public health systems, where a major proportion of medicines consumed is provided by the public health system, in India around 85% of medicines consumed are bought by patients from chemists shops.
Drug Price Control: Past Experience
While medicine prices have been controlled in some manner since 1962, the first comprehensive drug price control order (DPCO) was introduced in 1979. Since then, the DPCO was amended in 1987 and 1994. While in 1979, most medicines were brought under price control, amendments to the DPCO in 1987 and 1995 resulted in most drugs being removed from price control. (see Table)
Table: Change in Drug Price Control
|
DPCO Year |
No. of Drugs under Price Control |
Percent of Market Covered in Price Controlled Category (approx.) |
Mark-up (profitability) allowed |
| 1979 | 347 | 80-90% |
40%, 50% and 100% in three categories termed “life saving”, “essential” and “non essential” |
| 1987 | 142 | 60-70% | 75% and 100% in two categories, subsequently one category with 100% mark up |
| 1995 | 74 | 25-30%* | 100% |
*Even less now as many of the 74 drugs are now obsolete and just over 30 of the drugs in the price control list have any public health relevance
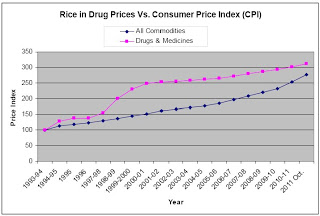
Thus, over time, the prices of an overwhelming majority of medicines in the market have been decontrolled. While the Government has continued to reason that such decontrol is necessary for the health of the industry, it has had a serious and continuous impact on drug prices – which have grown exponentially over time (see Chart below).
Chart: Price Rise in the Pharma Sector

DruDrDrug
Drug prices have risen in the past decades because of price decontrol and through manipulation of the market by pharmaceutical companies. That the market for medicines is rigged by drug companies is clear from the fact that top-selling brands of medicines are often the most expensive or one of the most expensive. This is clearly not a free market situation where competition helps stabilize prices, but a situation where large companies maintain high prices by bribing doctors and chemists to promote their more expensive medicines even though the same drug is available at 1/5th or 1/10th of the price charged by many top selling brands.
In 2002 a new drug policy was announced, that if implemented, would have further slashed the number of drugs under price control from the 74 in the 1994 policy. However a PIL challenged the policy in the Karnataka High Court on the grounds that it did not effectively control drug prices. The Karnataka High Court issued a stay on the implementation of this Policy. This order was challenged by the Government in the Supreme Court. The All India Drug Action Network joined this PIL in the Supreme Court which vacated the stay vide its order but observed:
“we suspend the operation of the order to the extent it directs that the Policy dated 15.2.2002 shall not be implemented. However we direct that the petitioner shall consider and formulate appropriate criteria for ensuring essential and life saving drugs not to fall out of the price control and further directed to review drugs, which are essential and life saving in nature till 2nd May, 2003”.
Since then there have been several calls for the introduction of a fair pharma pricing policy. These calls have also been echoed by the Parliamentary Standing Committee on Health and by the Supreme Court. The Government responded to such calls by constituting several Committees e.g the Sandhu Comitteee and the Pronob Sen Committee. A ‘Group of Ministers’ was constituted during the term of UPA I to effect a fair resolution of the issue. It remains a mystery why the group failed, in seven long years, to find a solution.
Safeguard for Industry, not for Peoples Health
It is in the above background that the draft Pharma policy, 2011 has to be seen. It has been formulated in a situation when: 1) Most medicines are outside price control; 2) There is complete anarchy as regards prices of medicines outside price control, with clear evidence that the same medicine is being sold at prices that vary enormously. 3) The prices of top selling brands of the same medicine are often the most expensive.
The proposed policy starts with a radical and welcome proposal that all drugs (348) in the National Essential Drug List brought be brought under price control. But this proposal hides a much more nefarious design that seeks to legitimize the rampant practice of profiteering in the pharmaceutical market. It does so by proposing that henceforth prices of medicines shall be fixed based on “market based” criteria. Till now, drug prices were fixed by using a ‘cost plus’ formula. The price of the finished product sold in the market was fixed by calculating the cost of manufacturing and then by placing a ceiling on the post manufacturing expense. The post manufacturing expense (MAPE) allowed included the profit for the company – as per the 1995 DPCO it stands at 100%. Thus if the cost to manufacture a formulation is Rs.1.00, it can be sold at Rs.2.00.
The new policy makes two significant departures from the existing methodology of calculating the price of a medicines.
1) It will only fix the prices of formulations (finished medicines sold in the market) and not of bulk drugs (raw material used to manufacture the finished product)
2) It will not use the earlier cost-plus formula but shall use what it calls “market based” pricing